Biomarkers are the little clues that keep oncology from turning into a guessing game. Think of them as the labels, receipts, and “this way please” signs cancer cells leave behind. Some point to what the disease is. Some hint at how it may behave. Others tell doctors which treatment is more likely to help.
That is the useful magic here: biomarkers help turn cancer treatment from a one-size-fits-everyone hallway into something closer to a map with a few extra street names. If you want broader site context, the homepage and Latest Lectures page collect related hematology material.
For readers who want the official version of this idea, the National Cancer Institute’s overview of biomarker testing for cancer treatment is a good starting point, and the FDA’s companion diagnostic guidance shows how test results can be tied to drug choices. The short version: the lab result is not just trivia. It can change the route.
What are biomarkers?
A biomarker is a measurable sign of a normal process, a disease process, or how the body is responding to treatment. In cancer, biomarkers can be genes, proteins, or other molecules found in blood, tissue, or marrow. The NCI defines biomarker testing as a way to look for those substances so doctors can better choose treatment.
Not every biomarker does the same job. Some are diagnostic, some are prognostic, and some are predictive. The names sound like they were invented by a committee that feared joy, but the roles are actually pretty practical.
| Type | Plain-English meaning | Why it matters |
|---|---|---|
| Diagnostic | Helps identify what disease or subtype is present | Supports the original diagnosis and helps separate one cancer from another |
| Prognostic | Suggests how the disease may behave over time | Helps estimate risk, even before a treatment is chosen |
| Predictive | Suggests which treatment is more likely to work | Guides therapy selection, especially for targeted drugs and immunotherapies |
| Monitoring | Shows whether disease is shrinking, staying quiet, or trying to sneak back in | Helps track response and relapse risk during or after treatment |
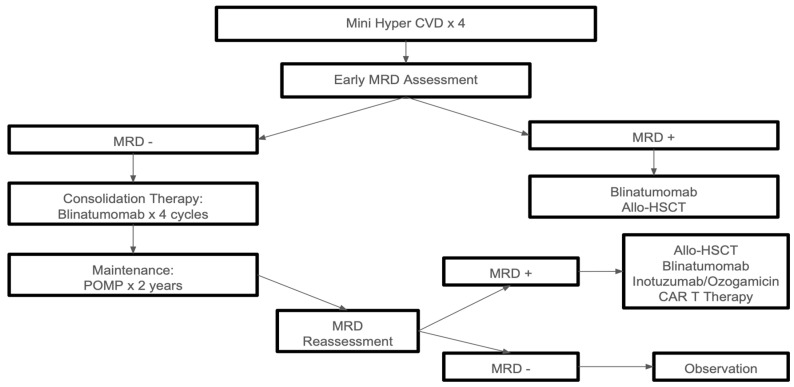
In blood cancers, monitoring often includes measurable residual disease, or MRD. The NCI notes that MRD testing is used mostly for lymphoma and leukemia, and that it can help plan treatment, judge response, and estimate whether cancer has returned.
MRD is the sneaky leftover stuff: the tiny number of cancer cells that may remain after treatment, even when the microscope looks reassuring. It is less “all clear” and more “let’s keep checking the shadows.”
How biomarkers influence treatment decisions
Biomarker testing usually begins with a sample from blood, bone marrow, or tumor tissue. That sample is then analyzed for genetic changes, protein patterns, or other signals. The result can affect whether the team uses standard chemotherapy, adds a targeted drug, or follows a different path altogether.
A practical way to think about the process:
- The sample arrives. Blood, tissue, or marrow goes to the lab.
- The lab looks for markers. This can include DNA changes, fusion genes, surface proteins, or protein overexpression.
- The result is matched to treatment options. Some findings point toward a specific drug class or a clinical trial.
- The plan is adjusted. The team may intensify treatment, de-escalate a bit, switch drugs, or monitor more closely.
The key phrase here is matched to treatment options. Biomarker testing does not tell the whole story, and it certainly does not replace clinical judgment. It acts more like a very well-informed assistant with excellent filing habits.
One useful example comes from the NCI’s adult acute lymphoblastic leukemia treatment guidance, which explains that the BCR::ABL1 fusion gene creates the Philadelphia chromosome. That biomarker matters because it can open the door to targeted therapy in Ph-positive ALL.
Another practical example is FLT3-altered acute myeloid leukemia. The NCI notes that adding an FLT3 inhibitor to induction chemotherapy is standard for eligible patients with FLT3-altered AML. That is biomarker-guided treatment in plain clothes: the lab result changes the drug list.
Key terms that keep the jargon from winning
Companion diagnostic
A companion diagnostic is a test that provides information essential for the safe and effective use of a corresponding therapy. In regular human language, it is the lab test that helps prove a drug is the right key for this particular lock.
Liquid biopsy
A liquid biopsy is a blood-based test that looks for tumor-derived material such as DNA fragments or cells. It is not a universal replacement for tissue testing, but it can be useful when repeated sampling is hard or when clinicians want another look without another procedure.
Surface marker
Some cancers show proteins on their outer surface. In B-cell lymphomas and leukemias, CD20 is a classic example. The NCI describes CD20 as a protein found on B cells that can help diagnose cancer or plan treatment, and it is one reason anti-CD20 therapies exist in the first place.
Prognostic vs. predictive
This pair gets mixed up constantly, so here is the sticky-note version. Prognostic biomarkers say something about the disease’s likely behavior. Predictive biomarkers say something about how a treatment is likely to perform. Same family, different job description.
Examples in hematological cancers
Blood cancers are where biomarkers really get to wear their name tag. The disease is often molecularly specific, which makes testing especially helpful.
| Example | What it tells the team | Why it matters |
|---|---|---|
| BCR::ABL1 in Ph-positive ALL or CML | A fusion gene created by the Philadelphia chromosome | Can point to targeted therapy with a tyrosine kinase inhibitor |
| FLT3 alterations in AML | A mutation or internal tandem duplication affecting a growth-signaling pathway | May support adding an FLT3 inhibitor to treatment |
| CD20 in B-cell lymphoma or leukemia | A surface protein on B cells | Can support use of anti-CD20 therapy such as rituximab in appropriate settings |
| MRD in leukemia or lymphoma | Tiny amounts of disease that may remain after treatment | Helps judge whether the current plan is working well enough or needs a pivot |
The point is not that every patient gets every test. The point is that the right test can narrow the field fast. Instead of asking, “What is cancer doing?” the team can ask, “What is this cancer doing, and what does that mean for treatment?” That is a better question with a better chance of a useful answer.
For a deeper look at blood-cancer biomarkers and treatment pathways, the NCI pages on adult ALL treatment, adult AML treatment, and tumor marker tests in common use are useful references.
Future of biomarker research
The future of biomarker research is moving in a few directions at once: broader genomic testing, better MRD tracking, more liquid biopsy use, and more precise matching of patients to therapy. NCI’s myeloMATCH program is one example of how biomarker-based treatment trials are being built for myeloid cancers.
That future is exciting, but it is not free of potholes. A better test is only useful if it is accurate, available, affordable, and interpreted correctly. If not, it becomes another shiny interface with a hidden error message.
Three challenges keep showing up:
- Access. Not every center has the same tests or turnaround times.
- Validation. A test has to be analytically sound before it can steer treatment.
- Interpretation. A biomarker result is a clue, not a prophecy.
The FDA has continued to refine how companion diagnostics are evaluated, which matters because oncology keeps getting more molecular and less “guess and hope.” That kind of structure helps make sure the test and the drug actually belong in the same sentence.
Conclusion
Biomarkers are not decorative lab jargon. They help identify cancers, estimate risk, and guide treatment choices that can be more precise than the old one-size-fits-all approach. In hematological cancers especially, biomarkers like BCR::ABL1, FLT3, CD20, and MRD can change what treatment is chosen and how response is monitored.
The practical takeaway is simple: if your care team mentions a biomarker, ask what it tells them, whether it is diagnostic, prognostic, or predictive, and how it changes the plan. That one question can turn a foggy appointment into a useful one.
And if you want a clean next step, ask the oncologist or hematologist, “Which biomarker matters most in this case, and what would a positive or negative result change?” It is a small question, but it tends to pull the whole treatment map into focus.