DC vaccination sounds technical, but the underlying idea is straightforward: teach the immune system what to look for, then let it do the hunting. That is the promise behind dendritic cell vaccination, and it is worth understanding carefully because the evidence is interesting, the limitations are real, and the practical questions are the ones patients and families actually live with.
If you are asking, “What exactly is a dendritic cell vaccine?”, “How does it differ from chemotherapy or checkpoint inhibitors?”, “What do the studies really show?”, and “What do patients experience during treatment?”, this article is for you. I am going to answer those questions in plain language, with the evidence kept in view rather than hidden in the margins.
The broader context matters too. On this site, the home page gathers the main lecture and article areas, while Latest Lectures is the place to look for related material on cancer treatment and immunology. For readers who want a basic, authoritative starting point, the National Cancer Institute’s overview of cancer treatment vaccines gives the clearest high-level summary I know.
DC vaccination is not a miracle cure, and no honest article should pretend otherwise. What it is, instead, is a different way of thinking about cancer treatment: rather than directly poisoning rapidly dividing cells, it tries to train the immune system to recognize a tumor as a target. That shift has produced one approved dendritic-cell-based treatment, has generated promising trial results in selected cancers, and has also produced some decidedly underwhelming studies. The story is better because it is mixed.
What DC Vaccination Is
“DC” stands for dendritic cell. The National Cancer Institute defines dendritic cells as special immune cells that help boost immune responses by showing antigens to other immune cells. In other words, they are not the soldiers; they are the officers who point the soldiers at the right target. That is why they matter so much in cancer immunotherapy.
A dendritic cell vaccine takes advantage of that role. Doctors collect cells, expose them to tumor material or tumor-specific antigens outside the body, encourage those cells to mature, and then return them to the patient. The goal is to make the immune system see cancer more clearly than it otherwise would. The NCI notes that dendritic cell vaccines stimulate the immune system to respond to antigens on tumor cells, and that one dendritic cell vaccine, sipuleucel-T, is already approved for some men with advanced prostate cancer. That definition matters because it explains why DC vaccination sits between classic vaccination and cancer therapy: it is therapeutic, not preventive.
Here is the simplest way to think about the difference between DC vaccination and traditional treatment:
| Approach | What it tries to do | Main trade-off |
|---|---|---|
| Chemotherapy | Kill fast-growing cells directly | Can damage healthy tissue that also divides quickly |
| Checkpoint inhibitors | Release immune brakes already in place | Works well in some tumors, not all, and can trigger immune side effects |
| DC vaccination | Present tumor antigens and train T cells to recognize them | Personalized, labor-intensive, and still uneven in clinical benefit |
The plain-English conclusion is that DC vaccination is a training strategy. It is meant to improve the quality of the immune response rather than simply increase its volume.
Key terms in plain English
- Antigen: a molecular marker the immune system can recognize.
- Autologous: made from the patient’s own cells.
- Neoantigen: a tumor-specific target that arises from a cancer mutation.
- Antigen-presenting cell: an immune cell, such as a dendritic cell, that shows antigens to T cells.
- T cell: an immune cell that can help coordinate or directly attack abnormal cells.
Mechanism of Action
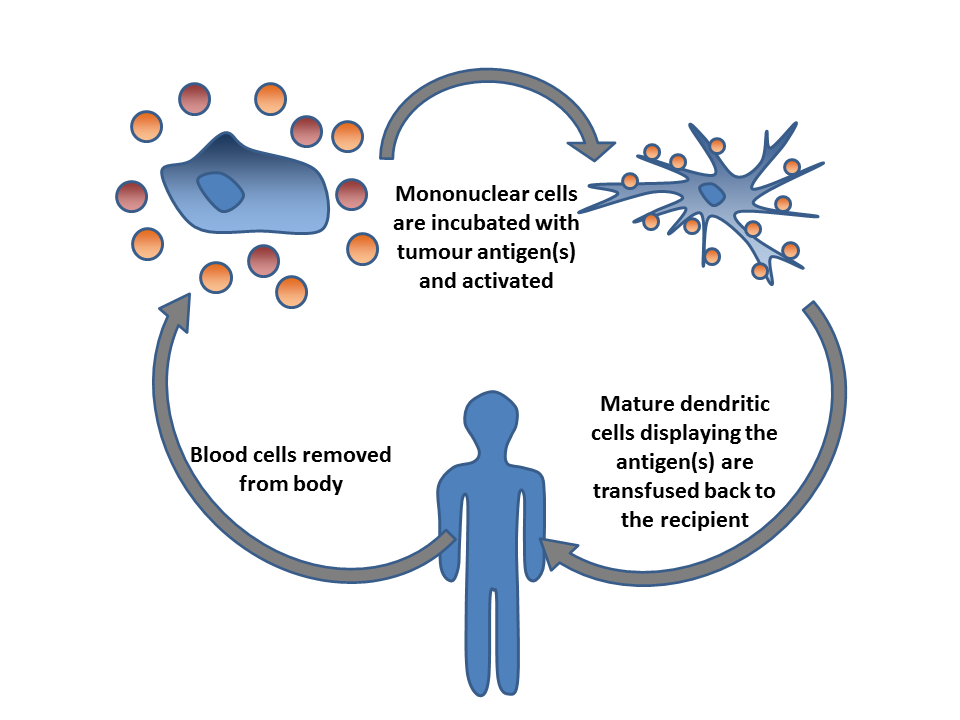
The mechanism is easier to follow if you treat it as a sequence rather than a slogan. When people say “DC vaccine,” they are usually talking about a personalized process with several steps, not a simple injection from a shelf.
- Cells are collected. Blood is drawn and immune cells are separated, often by leukapheresis.
- Dendritic cells are prepared in the lab. The cells are exposed to tumor antigens, tumor lysate, peptides, or other target material.
- The cells are matured. Immune-stimulating signals help them become better at activating T cells.
- The vaccine is returned to the patient. The treated cells are infused or injected back into the body.
- T cells are activated. If all goes well, T cells learn to recognize tumor cells carrying the same target.
- The immune system expands the response. Ideally, the tumor becomes easier to find and harder to hide from.
That sounds tidy on paper. Biology is less cooperative.
For a vaccine like this to work, several things have to line up at once: the tumor has to have a useful target, the dendritic cells have to be properly activated, the T cells have to reach the tumor, and the tumor microenvironment has to be less suppressive than it often is. Cancer is excellent at discouraging exactly the immune response it wants to avoid. That is one reason the results are promising but inconsistent.
There is also a comparison worth making with checkpoint inhibitors. Checkpoint drugs such as PD-1 or PD-L1 blockers help immune cells act after they already recognize a target. DC vaccination tries to improve the recognition step itself. In that sense, the two approaches are complementary rather than redundant. They are different doors in the same corridor.
Researchers have increasingly focused on personalized antigen selection, especially neoantigens. A 2024 PubMed review on personalized dendritic-cell-based vaccines targeting neoantigens argues that the field is moving toward more precise antigen choice, which makes biological sense: the more specifically the vaccine matches the tumor, the less likely it is to waste effort on the wrong target.
Recent Research Findings
If I had to compress the recent literature into one sentence, it would be this: DC vaccination remains biologically credible, clinically uneven, and most interesting when it is personalized.
The first point of reference is the approved product sipuleucel-T. The NCI describes it as a dendritic-cell vaccine used for some men with advanced prostate cancer, and its existence matters because it proves the concept reached the clinic rather than stopping at theory. That does not make every DC vaccine effective, but it does make the platform real.
Beyond that approval, the research picture is more mixed. Recent reviews and trials show three recurring themes:
- Safety is often acceptable. Many studies report mostly mild or manageable side effects, though the exact profile depends on the protocol and cancer type.
- Immune responses are easier to show than survival gains. A vaccine may clearly activate the immune system without producing dramatic tumor shrinkage.
- Patient selection matters. The strongest signals tend to appear in settings where the tumor burden is lower, the antigens are better defined, or the vaccine is integrated with other therapies.
A 2024 PubMed review of dendritic cell vaccines for glioblastoma is a useful example of the field’s cautious optimism. Glioblastoma remains one of the hardest cancers to treat, yet DC vaccine studies continue because they sometimes show survival or immune signals worth pursuing. The point is not that the problem is solved. The point is that the idea keeps surviving contact with reality.
Another 2024 review, also on PubMed, looked at personalized dendritic-cell vaccines and emphasized the growing role of neoantigens. That is a meaningful shift. Older vaccine strategies often used broad tumor material and hoped the immune system would find something useful inside. Newer strategies try to be more deliberate. Precision tends to be boring only until it starts working.
Recent trial data also suggest that the context matters more than the headline. In some studies, DC vaccination has been associated with prolonged survival or disease control; in others, the clinical effect has been modest or absent even when immune activation was measurable. A systematic review of cell-based cancer vaccines in 2024 found that many trials were still disappointing overall, which is a useful corrective against hype. The right conclusion is not that DC vaccination failed. It is that the field has learned where the rough edges are.
When I look at the literature as a whole, the pattern is familiar to anyone who has watched immunotherapy mature: a promising mechanism, a useful approved example, a lot of engineering pain, and a long list of details that decide whether a trial becomes a real therapy or just another hopeful graph.
What the evidence seems to favor
- Personalized antigen selection rather than one-size-fits-all targets.
- Better integration with other immunotherapies instead of using DC vaccines in isolation.
- Careful attention to who is enrolled, when they are treated, and what outcome is being measured.
Patient Experiences
This is the section that often gets flattened into vague optimism, so I want to keep it specific. Published patient experiences with DC vaccination are usually not dramatic testimonials. They are quieter than that, and in some ways more useful.
A 2023 qualitative study on attitudes, expectations, and lived experiences of cancer patients receiving dendritic cell vaccine therapy in Japan found that patients often approached the treatment with hope, curiosity, and some uncertainty about whether it would help. That combination is easy to understand. The treatment is personalized and high-tech, but the uncertainty around benefit is still real. People do not become irrational just because a treatment sounds futuristic.
From a practical standpoint, patients often describe the logistics as part of the experience:
- blood collection or cell harvesting before treatment,
- waiting for the vaccine to be manufactured,
- repeated visits for injections or infusions,
- monitoring for side effects and disease response.
That makes DC vaccination different from taking a tablet at home and hoping for the best. It asks more of the patient’s time, patience, and schedule. The upside is that many patients find the therapy less physically punishing than standard chemotherapy. In studies of metastatic prostate cancer and other settings, health-related quality of life stayed high during DC-based immunotherapy, which is an important result even when response rates are modest. A treatment does not need to be dramatic to be valuable, but it does need to respect the patient’s daily life. That is not a luxury criterion. It is the job.
There are also studies in which patients reported improvements in appetite, sleep, strength, or overall wellbeing during DC-based treatment. One colorectal cancer study reported improvements in physical strength, appetite, sleep, and body weight, with fever and insomnia among the more common side effects. That is a useful reminder that “experience” is not just about tumor scans. It is also about whether a person can keep eating, sleeping, and making it through the week without the treatment becoming the central event of every day.
So if someone asks, “What do patients think of dendritic cell vaccination?”, the honest answer is: many of them see it as hopeful, personalized, and tolerable, but they also live with uncertainty about whether the treatment will translate into meaningful cancer control. That is not a flaw in patient perception. It is the reality of the evidence.
A practical summary of patient-reported experience
| What patients often notice | What it means in practice |
|---|---|
| Hope from a personalized approach | The treatment feels tailored rather than generic |
| Logistical burden | Manufacturing time, repeat visits, and monitoring are part of the course |
| Often manageable side effects | Many studies report mild reactions, though this depends on the protocol |
| Uncertain payoff | Some patients benefit clearly; others do not |
What This Means for Patients and Clinicians
There are a few practical conclusions worth carrying forward.
- DC vaccination is best understood as a personalized immunotherapy platform. It is not a general-purpose substitute for all other cancer treatments.
- The strongest results tend to come from carefully selected settings. Tumor type, stage, antigen choice, and combination strategy all matter.
- Safety and quality of life are part of the real value proposition. A treatment that preserves daily function may be meaningful even when it is not curative.
- The evidence base is promising but not settled. That sentence is less exciting than hype, and far more useful.
If you or someone close to you is considering a DC vaccine, the right questions are practical ones: What antigen is being used? Is this part of a trial? What is the evidence in this exact cancer type? What side effects are expected? How long does manufacturing take? What happens if the disease progresses while the vaccine is being prepared? Those are not pessimistic questions. They are the questions that keep hope tethered to reality.
Why the evidence stays mixed
One reason DC vaccination has not become routine across cancer care is that the therapy depends on timing. By the time a vaccine is manufactured and the patient is ready to receive it, the disease may already have changed. Tumors evolve quickly, and the immune system is forced to play catch-up. That does not make the approach pointless; it makes it conditional. The most persuasive use case is often as part of a broader plan, after surgery or alongside other immune therapies, when the target is still clear and the patient can wait long enough for the personalized product to matter.
Manufacturing quality also matters more than most people realize. A dendritic cell vaccine is not a single molecule synthesized on a factory line. It is a process. If the starting cells are poor, the antigen selection is weak, or the maturation step is inconsistent, the final product may be biologically active in theory but underpowered in practice. That is one reason recent papers keep returning to the same themes: better antigen choice, better standardization, and better combination strategies. The science is not short on imagination. It is short on tolerance for sloppy execution.
There is also an important research question that has not gone away: which cancers are most likely to benefit? In the literature so far, some of the more active areas include prostate cancer, glioblastoma, melanoma, renal cell carcinoma, and certain hematologic cancers. But “active research area” is not the same thing as “proven standard of care.” The distance between those two phrases is where the hard work happens.
Conclusion
Dendritic cell vaccination is one of the more intellectually satisfying ideas in cancer immunotherapy because the logic is elegant: show the immune system the target, improve the response, and let biology do more of the work. The reality is less tidy, which is exactly why the subject remains interesting. Some patients benefit. Some trials disappoint. Some studies show immune activation without clear clinical payoff. And yet the platform keeps evolving, especially as researchers move toward personalized neoantigen selection and better combination strategies.
So the useful takeaway is not “this is the answer” or “this has failed.” It is this: DC vaccination is a credible, evolving approach that has already produced one approved therapy and continues to generate serious research, but its benefits depend heavily on the cancer, the patient, and the design of the vaccine itself.
If you want to keep following the topic, start with the broader context on the home page, then browse the Latest Lectures archive for related material. That is usually a better next step than chasing the loudest headline. Cancer treatment rarely rewards headlines. It tends to reward specificity.
Key points to remember:
- DC vaccination trains dendritic cells to present tumor antigens to T cells.
- The approach is personalized and often more logistically involved than standard treatment.
- Evidence is strongest when antigen choice is precise and patient selection is careful.
- Patient experiences often highlight hope, tolerability, and uncertainty at the same time.
- The field is promising, but it is still working through the practical limits of biology and manufacturing.